유방암 환자에서 유방보존술 후 무세포 진피조직을 이용한 재건과 일차적 봉합 사이의 비교
Comparison of Wound Closure Using Acellular Dermal Matrix With Primary Wound Closure After Breast Conserving Surgery in Breast Cancer Patients
Article information
Trans Abstract
Purpose
As breast-conserving surgery has become a standard treatment for patients with breast cancer, several approaches have been devised to achieve desirable cosmetic results, including a method using a patient’s own tissues or organs or a mesh to resolve defects. However, its application has been limited due to the associated complications. Accordingly, breast reconstruction using an acellular dermal matrix (ADM) has been introduced to improve patients’ cosmetic satisfaction. However, the comparison of reconstruction and primary sutures using this method has not been well-studied. Therefore, this study surveyed patients who underwent breast cancer surgery based on cosmetic indicators to study the efficacy of ADM after breast-conserving surgery.
Methods
This retrospective study included 68 patients diagnosed with breast cancer who underwent breast-conserving surgery at a single institution by a single surgeon from April 2019 to December 2020.
Results
This study included 68 patients who underwent breast-conserving surgery. Among them, 22 patients underwent breast-conserving surgery using ADM, while 46 patients received only primary sutures without ADM. Among the items of the Breast Cancer Treatment Outcome Scale-12 (BCTOS-12), patient satisfaction was significantly higher in the group using ADM, than that in the control group in terms of breast shape (1.86±0.89 vs. 2.39±0.80, p=0.017). Regarding breast tenderness, the result also confirmed the group treated using ADM experienced less tenderness than the control group not treated with ADM (1.68±0.78 vs. 2.22±1.03, p=0.035). The two groups exhibited no significant differences in breast texture, arm heaviness, nipple appearance, shoulder discomfort, arm discomfort, scar tissue, arm swelling, breast swelling, fit of the bra, and breast sensitivity.
Conclusion
Breast reconstruction using ADM in patients with breast cancer was effective from a cosmetic perspective. Prospective multicenter studies should be conducted to provide clear guidelines.
서 론
유방보존술은 현재 유방암의 국소-구역치료의 표준적인 치료로 자리 잡고 있다. 유방보존치료에 대한 임상시험은 이전부터 시작되었고, 이러한 임상시험들을 메타 분석한 결과에서 유방보존술 후에 방사선 요법을 시행하는 것은 유방절제술과 비교하였을 때 동등한 장기 생존율을 보였다[1].
이렇게 유방보존술이 유방암 환자에서 표준 치료로 자리 잡게 되면서 미용적으로 좋은 결과를 얻을 수 있도록 하는 여러 방법들이 고안되었고, 절제 이후 결손 부위를 해결하기 위해 유방실질을 이용하는 피판 이동술(glandular remodeling)만으로 만족할 만한 결과를 얻기 힘든 경우 주변조직 또는 원격장기를 이용하는 피판 치환술과 같은 종양 성형술의 개념 또한 등장하게 되었다[2].
특히 한국인 및 아시아계 여성들은 서양 여성에 비해 유방의 전체 부피는 작으나, 종양의 크기는 상대적으로 커서[3-5], 환자 자신의 조직만으로 피판 이동을 하여, 미용적 만족을 얻기에는 한계가 있어왔다.
무세포 진피조직(acellular dermal matrix, ADM)은 콜라겐(collagen), 엘라스틴(elastin), 프로테오글리칸(proteoglycan), 라미닌(laminin) 그리고 기저막(basement membrane)으로 구성되어 있는데, 이들은 재상피화 및 혈관 신생에 도움을 주고, 면역 반응을 일으키지 않아 화상관리 및 재건수술에 많이 사용되고 있다[6-8].
ADM이 유방수술에 적용된 예로는 유방 전 절제 후 보형물을 이용한 재건 시 유방하부의 피하 포켓을 보강할 필요가 있을 경우 사용할 수 있다고 언급되었으나[9], 직접적으로 유방보존술 시 유방 모양 변형을 막기 위한 미용적인 목적으로 사용된 예는 많지 않다.
따라서 본 연구의 목적은 본원에서 유방보존술을 받은 유방암 환자들의 자료를 바탕으로 ADM 사용군과 일차적 봉합군 사이에서 환자의 미용적인 만족도를 설문조사하여, 수술 후 경과에 차이가 있는지 분석하고자 하였다.
방 법
대상 및 연구 자료
2019년 4월부터 2020년 12월까지 단일 기관, 단일 술자에 의해 유방암으로 수술을 받은 환자들의 의무 기록 및 검사 결과 등 기존의 자료를 후향적으로 비교 분석하고, 설문조사를 시행하였다.
총 98명의 환자가 있었으나, 이중 22명은 유방 전 절제술을 시행하였으므로, 결과 분석에서 제외되었고, 유방보존술을 시행한 76명을 대상으로 하였다.
이 중 미용적인 만족도 설문조사에 응하지 않은 환자 1명, 양측 유방 수술을 시행한 환자 7명을 제외하고 총 68명의 환자가 포함되었으며, 연령, 성별, 수술일자, 병기, 검체 크기, 원발암 크기 등을 조사하여 ADM 사용에 따른 각 미용적 변수 간의 차이가 있는 지를 알아보고자 하였다(Table 1).

Baseline characteristics of treated patients
본 연구는 순천향대학교 부속 천안병원 임상 연구 심의위원회(Institutional Review Board)의 승인을 받았다(IRB No. SCHCA 2021-02-017).
수술 방법
유륜 주변으로 인디고카민(indigo carmine)을 주입하고 5분 정도 마사지를 시행한 뒤, 겨드랑이에 약 3 cm 가량의 절개를 가하여 염색되어 있는 림프절을 확인하고 이를 생검하여 동결 조직 검사를 시행하였다. 이후 초음파로 병변의 위치를 확인하여 유방에 절개선을 그리고 절개선을 따라 지방과 조직을 절개해 나간 뒤, 대흉근 및 소흉근까지 표시된 선을 따라 절개 후 검체를 떼어내었다(Figure 1). 검체의 가장자리를 봉합사로 표시한 뒤 암 침범 여부를 확인하기 위해 동결조직 검사를 시행하였고, 조직 검사 상 가장자리에 병변이 가까울 경우에는 추가적인 절제를 시행하고 재검사하였다. 이후 절제된 결손부위에 맞게 ADM을 재단한 뒤(Figures 2, 3) 단일필라멘트 흡수 봉합사(monofilament absorbable suture)로 주변 조직과 고정하였다(Figure 4). 이후 겨드랑이와 유방실질을 절제한 곳으로 배액관을 거치하고 피부 봉합 후 수술종료 하였다(Figure 5). ADM을 사용하지 않은 그룹은 상기 서술한 방법과 동일하게 진행하였으나 ADM을 사용하지 않고, 피판 이동술을 이용하여 유방실질을 봉합하거나 실질의 봉합 없이 배액관 거치 후 단순 피부 봉합을 하였다.

Defects after lumpectomy. As the mass was removed, a defect was created in the breast parenchyma.

Acellular dermal matrix. The acellular dermal matrix was prepared aseptically.

Remodeling of acellular dermal matrix. The acellular dermal matrix was designed according to the shape of the defect in the patient’s breast.
Application of acellular dermal matrix. The acellular dermal matrix was inserted into the patient’s breast and fixed to the surrounding breast tissue with monofilament absorbable suture.

Post-operative finding. After the drainage tube was placed, the operation was completed, and the defect in the breast was corrected through the use of acellular dermal matrix.
분석방법 및 통계기법
본 연구에서는 ADM으로 결손 보강을 한 그룹과 하지 않은 그룹을 비교하기 위해 환자들의 만족도 평가인 Breast Cancer Treatment Outcome Scale-12 (BCTOS-12)를 사용하였다. 초기엔 22가지 항목으로 구성된 Breast Cancer Treatment Outcome Scale-22 (BCTOS-22)였으나 수렴적 타당성이 우수한 BCTOS-12로 축소 개량되어 쓰이고 있다[10].
이 평가는 유방보존술 이후 미용적, 기능적 상태를 평가하는 12개의 항목으로 구성되어 있으며, 이는 1) 유방의 모양(breast shape), 2) 유방의 질감(breast texture), 3) 팔의 무게감(arm heaviness), 4) 유두의 모양(nipple appearance), 5) 어깨의 불편함(shoulder discomfort), 6) 팔의 불편함(arm discomfort), 7) 유방의 압통(breast tenderness), 8) 흉터(scar tissue), 9) 팔의 붓기(arm swelling), 10) 유방의 붓기(breast swelling), 11) 속옷의 맞는 정도(fit of bra), 12) 유방의 감각(breast sensitivity) 으로 이루어져 있고, 기능적인 항목과 미용적인 항목으로 구분이된다(Table 2).
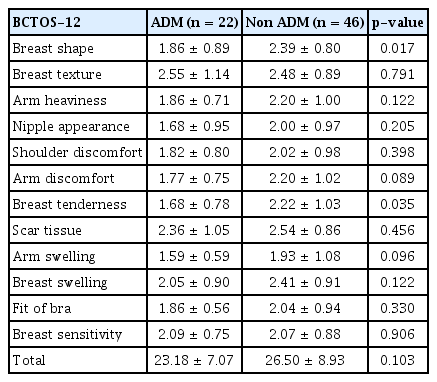
Comparison of outcome between two groups
기능적인 항목은 1) 팔의 무게감, 2) 어깨의 불편함, 3) 팔의 불편함, 4) 팔의 붓기, 4가지 항목으로 나누어져 있고, 미용적인 항목은 나머지 8가지 항목으로 구성되는데, 1) 유방의 모양, 2) 유방의 질감, 3) 유두의 모양, 4) 유방의 압통, 5) 흉터, 6) 유방의 붓기, 7) 속옷의 맞는 정도, 8) 유방의 감각으로 나누어져 있다.
각각의 항목은 1점부터 4점까지 치료를 하지 않은 반대쪽 유방과 비교하여, 환자의 주관적인 만족도에 따라 답변을 할 수 있도록 되어 있으며, 점수가 높을수록 낮은 만족도를 나타내게 된다[11].
이상에서 수집된 자료를 바탕으로 후향적 비교 분석을 시행하였다. 연속형 변수는 t-검정 혹은 Mann-Whitney U 검정을 시행하여 p-value를 산출하고 결과값은 평균±표준편차의 값으로 제시하였으며, 범주형 변수에 대해서는 카이제곱 검정 혹은 Fisher의 정확검정(Fisher’s exact test)를 시행하여 p-value를 산출하였으며 결과값은 빈도로 제시하였다. p-value는 0.05 미만을 통계학적으로 유의한 것으로 정의하였으며 통계분석은 the SPSS software (Version 23.0; IBM Co., Armonk, USA)을 이용하였다.
결 과
유방암 수술 중 유방보존술을 시행받은 68명의 환자가 포함되었으며, 이중 22명은 ADM을 사용한 유방보존술을 시행받은 군이었으며, 46명이 ADM 없이 일차봉합만 시행 받은 군이었다.
ADM을 사용한 군의 평균 나이는 48.05±9.76세였으며, ADM을 사용하지 않은 군의 평균 나이는 53.02±10.14세 로 두 군 간의 유의한 차이는 없었다. American Joint Committee on Cancer (AJCC) 8판에 의한 병기 분류상 ADM을 사용한 군에서 각각 0기 2명(9.0%), 1기 10명(45.5%), 2기 9명(40.9%), 3기 1명(4.5%)이었으며, ADM을 사용하지 않은 군은 각각 0기 13명(28.3%), 1기 13명(28.3%), 2기 19명(41.3%), 3기 1명(2.2%)으로 병기 분포에도 유의한 차이는 보이지 않았다(Table 1).
수술일로부터 BCTOS를 시행한 날까지의 기간을 비교하였을 때 ADM을 사용한 군은 445.27±126.62일이었고, ADM을 사용하지 않은 군은 421.52±191.94일로 유의한 차이를 보이지 않았으며, 각 군의 중위값 및 범위는 447.5일(137-745), 453일(109-743)이었다.
ADM을 사용한 군에서 각각 에스트로겐 수용체 양성은 17명(77.3%), 음성은 5명(22.7%)이었고, 프로게스테론 수용체 양성은 14명(63.6%), 음성은 8명(36.4%)이었으며, 대조군에서 에스트로겐 수용체 양성은 35명(76.1%), 음성은 11명(23.9%), 프로게스테론 수용체 양성은 33명(71.7%), 음성은 13명(28.3%)이었다. 호르몬 수용체 분포에서도 두 군 사이에 유의한 차이는 없었다(Table 1).
HER-2 수용체 유무에서도 ADM을 사용한 군에서 양성 3명(13.6%), 음성 19명(86.4%)이었고, 일차봉합을 한 군에서는 양성 6명(13.0%), 음성 40명(87.0%)으로 유의한 차이는 없었다.
검체의 크기는 ADM을 사용한 군에서 7.16 ±1.50 cm였으며, ADM을 사용하지 않은 군의 검체 크기는 6.75±1.62 cm이었다.
ADM을 사용하면서 삽입부위의 감염은 총 22명의 환자 중 1명(4.5%)이 경험하였다. 기저질환으로 당뇨가 있는 환자였으며 수술 후 열흘 정도 후 발생하였으나, 드레싱 유지 후 호전되었다.
68명의 환자들에게 각각 만족도를 조사하였을 때, BCTOS-12의 항목 중 유방의 질감, 팔의 무게감, 유두의 모양, 어깨 불편감, 팔의 불편감, 흉터, 팔의 붓기, 유방의 붓기, 속옷의 맞는 정도, 유방 감각에서는 두 군 간의 유의한 차이가 없었다(Table 2). 그러나 유방의 모양에서는 ADM을 이용한 군에서 그렇지 않은 대조군에 비해 환자들의 만족도가 높았으며(1.86± 0.89 vs. 2.39± 0.80, p= 0.017), 유방의 압통에서도 ADM을 이용한 군에서 그렇지 않은 대조군에 비해 압통이 덜했음을 확인할 수 있었다(1.68± 0.78 vs. 2.22±1.03, p= 0.035).
하지만 기능적인 항목 및 미용적인 항목을 종합적으로 고려하였을 때는 두 군 간의 유의한 차이가 없었다(functional score: 7.05± 2.26 vs. 8.35± 3.62, p = 0.075, cosmetic score: 16.14± 5.37 vs. 18.15± 5.89, p= 0.179) (Table 3).

Comparison of functional score and cosmetic score
고 찰
Fisher 등[9]에 의해 유방보존술 후 방사선 치료의 안정성이 입증된 이후로 유방 보존에 대한 관심은 지속적으로 유지되어 왔으며, 이에 따른 수술 방법 및 안정성에 대한 연구도 계속되어 왔다[2].
특히 한국의 경우 2000년에는 6천여 명을 약간 넘던 유방암의 발생이 꾸준히 늘어나 2018년에는 2만 8천여 명을 상회하고 있고, 발생 연령대가 서구화 되어가고 있다고는 하나 아직까진 비교적 젊은 환자에서 발생이 많고, 검진의 발달로 조기 유방암의 빈도가 늘어남에 따라 유방보존술은 자연스럽게 늘어나 최근에는 전체 수술의 60% 이상을 차지하고 있다[12].
따라서 환자 개개인의 특성에 맞는 유방보존술의 방법에 대해서도 다양한 방법이 고안되었으며, 암을 완전히 절제하면서도 미용적인 특성을 고려하는 종양성형적 수술(oncoplastic surgery)의 개념을 도입하여 많은 수술이 개발되었다[2,3,13].
하지만 복횡근(transverse rectus abdominis muscle)이나 광배근(latissimus dorsi muscle)과 같은 근육을 이용하거나 임플란트(implant)를 이용한 유방보존술은 수술 시간도 오래 걸리고, 새로운 절개창을 가해야 하는 경우가 많고, 유방을 전 절제해야만 하는 경우가 많아 작은 결손을 위한 수술에 적합하지 않은 경우가 발생한다[2,14].
이에 국소적인 결손을 해결하기 위해 유방의 부분 절제 후 메쉬를 삽입하는 재건술 등이 대두되었으나, 유방보존술만 시행한 경우보다 상처감염이 더 많이 발생한다는 보고도 있고, 장액종 및 출혈 등의 합병증도 많은 것으로 나타났으며, 삽입 부위의 심각한 감염 발생 시 메쉬의 제거가 곤란한 경우가 생길 수 있어 이에 따른 장기간의 치료 및 사용에 제한이 있어왔다. 또한 1년 이상의 추적관찰을 하는 동안 재발이 발생할 경우 이의 구별이 쉽지 않다는 보고도 있었다[15-17].
본 연구에서는 이러한 작은 결손의 보완을 위해 오랫동안 의학분야에서 사용되어 온 ADM을 이용한 유방보존술에 대해 연구를 진행하였다. ADM은 주로 사체(cadever) 피부를 통하여 얻어지며, 방사선 처리를 통하여 표피 및 피부세포는 제거하고, 세포외기질(extracellular matrix)의 생화학적, 그리고 구조적인 특성(콜라겐, 앨라스틴, 프로테오글리칸 등)을 모두 살려 조직의 재생을 촉진하는 것으로 되어 있다. 특히, 화상 환자의 피부 이식분야에서 많이 이용되어 왔으며, 유방의 재건이나 탈장 등의 수술에도 이용되어 왔다[6,18].
그 동안 유방 전 절제술 후 임플란트를 넣기 전 보강을 위한 용도로 ADM이 사용되어진 보고는 있으나 결손부위에 직접 삽입하여 보강을 한 예는 많지 않다[19].
Kim 등[20]은 ADM의 안정성에 대한 연구에서 세포 독성이 적어 임플란트를 이용하는 유방보존술에 적합하다고 보고하였고, Wilson [21] 역시 유방보존술에서 임플란트를 삽입하기 전 ADM으로 보강을 하는 것이 육안적 및 조직학적으로 보강을 하지 않은 그룹보다 합병증 발생이 적은 것으로 주장하였다.
본원에서는 유방의 모양에 대한 평가에서 ADM을 이용한 군에서 그렇지 않은 대조군에 비해 환자들의 만족도가 높은 것으로 나타났는데(1.86± 0.89 vs. 2.39± 0.80, p = 0.017), 이는 작은 결손에 대한 ADM의 미용적인 측면에서는 환자들의 만족도를 높이는 유용한 방법이 될 수 있음을 나타냈다.
또한 유방의 압통을 조사한 항목에서 ADM을 사용한 군이 통증이 덜함을 확인할 수 있었는데(1.68± 0.78 vs. 2.22±1.03, p = 0.035), 이는 ADM을 사용함으로써 주변 조직을 덜 건드리게 되어 긴장도의 감소로 인한 효과로 유추해 볼 수 있겠다[22].
BCTOS-12 항목에는 없었지만 일부에서는 ADM을 삽입한 부위가 단단하게 만져지는 느낌이 있다고 호소하는 환자들이 있었는데, 이는 원래의 유방실질과 지방조직보다는 피부조직이 갖는 한계로 판단되나 장기간의 추적관찰을 통해 좀 더 연구해 볼 필요가 있을 것으로 사료된다.
또, 1예에서 당뇨를 기저질환으로 앓던 환자에서 열흘 정도 후 상처부위 감염이 발생하였으나 ADM의 제거 없이 드레싱으로 해결이 되었다. 다만 이 연구에는 포함되지 않았지만 연구 기간 후에 ADM을 사용한 기저질환이 없던 1명의 환자에서 상처부위 감염이 발생하여 드레싱 처치를 하였으나 상처부위의 열개(wound dehiscence)로 ADM을 제거하였으며, 제거 시 조직이 남는 등의 어려움은 없었다.
결론적으로 본 연구 결과는 유방보존술 이후 ADM의 사용이 환자의 유방의 모양 측면에서 미용적 만족도를 높이는 유용한 방법임을 보여주고 있다. 그러나 본 연구는 후향적 연구라는 점, 단일 기관, 단일 술자 연구로 모집단 수가 적다는 점, 장기간의 추적 관찰 결과가 아직 없다는 점에서 이 결과만으로 명확한 기준을 제시하는 데는 어려움이 있다. 따라서 앞으로 유방보존술을 시행 받는 환자에서 ADM 사용 여부를 결정하기 위한 전향적 무작위 배정 다기관 연구가 필요할 것으로 보인다.
Notes
The authors declare that they have no competing interests